Osteoarthritis is the most common form of arthritis. And because of this, I think it’s often dismissed, and its effects underestimated.
I mean, how often have you heard people say, ‘it’s just wear and tear’, ‘we’ll all get it eventually’, or my personal favourite ‘it’s just a bit of arthritis’ 😤? These offhand comments trivialise the considerable pain and disability that osteoarthritis (OA) causes many Australians.
If you have OA or know someone who does, you know it can significantly impact every aspect of life. Symptoms such as persistent pain, fatigue, stiff and swollen joints, weakened muscles, anxiety, depression, and sleep problems can affect a person’s ability to be as involved in social, community and work activities as they might like.
So, no, it’s not ‘just’ arthritis.
Let’s look at what it is.
What is osteoarthritis?
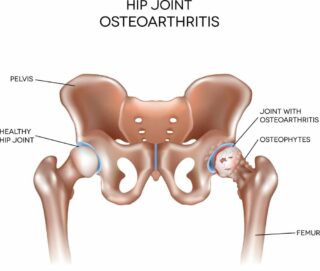
As we know, OA is the most common form of arthritis. It’s most likely to develop in people over 45, but it can also occur in younger people. It frequently affects weight-bearing joints, such as the knees, hips, feet, and spine. The joints of the hands, including the thumbs, are also commonly affected.
While it was once thought to be an inevitable part of ageing, resulting from a lifetime of wear and tear on joints, we now know it’s a complex condition and may occur due to many factors.
Osteoarthritis and your joints 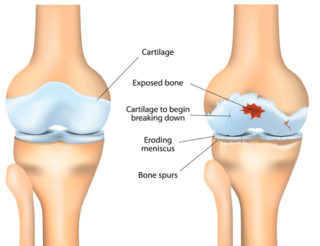
To understand how OA affects your body, it’s helpful to know a little about your joints.
Joints are places where bones meet. Bones, muscles, ligaments and tendons work together so you can twist, bend and move about.
Covering the ends of your bones is a thin layer of tissue called cartilage. It provides a slippery cushion that absorbs shocks, helps your joints move smoothly and prevents bones from rubbing against each other.
Around most of your joints is a tough capsule that holds your bones in place. The inside of the capsule is lined with synovial membrane, which produces synovial fluid. This fluid lubricates and nourishes the cartilage and other structures in the joint.
With OA, the cartilage becomes brittle and breaks down. Some pieces of cartilage may even break away and float in the synovial fluid. Because the cartilage no longer has a smooth surface, the joint becomes stiff and painful to move.
Eventually, the cartilage can break down so much that it no longer cushions the two bones. Your body tries to repair this damage by creating extra bone. These are bone spurs (or osteophytes). Bone spurs don’t always cause symptoms but can sometimes cause pain and restrict joint movement.
OA causes and risk factors
Many things can increase your chances of developing OA, including:
- your age – people over 45 are more at risk
- being overweight or obese
- your genetics – the genes you inherit can play a role in developing OA
- other conditions – such as rheumatoid arthritis and gout, can cause damage to your joints and lead to OA
- gender – 3 in 5 people who have OA are women
- repetitive movements associated with your job or occupation (e.g. constant kneeling, squatting, lifting heavy loads)
- significant injury, surgery, damage or overuse of a joint.
Signs and symptoms
The symptoms of OA can vary from person to person. Some of the more common symptoms include:
- joint pain, stiffness and swelling (inflammation)
- grinding, rubbing or crunching sensation (crepitus)
- muscle weakness.
These symptoms can sometimes worsen, especially when you feel stressed, upset, overdo things, or don’t get enough sleep. This is called a flare or flare-up.
Diagnosing OA
If you’ve been experiencing joint pain, it’s essential you discuss your symptoms with your doctor. Getting a diagnosis as soon as possible means that treatment can start quickly. This will give you the best possible outcomes.
To diagnose your condition, your doctor will do some exams or tests. They may include:
- Your medical history. Your doctor will ask you about your symptoms, family history and other health issues.
- Physical examination. Your doctor will look for swelling in and around the joint and test your joint’s range of movement. They’ll also feel and listen for grinding, rubbing or creaking in the joint.
Imaging (e.g. x-rays, ultrasound or MRI) and blood tests aren’t routinely used to diagnose OA. However, they may sometimes be needed if there’s uncertainty around your diagnosis.
Treating OA
There’s no cure for osteoarthritis; however, your symptoms can be effectively managed with exercise, weight management, medicines, and self-care.
Exercise
Because of the old ‘wear and tear’ myth, many people are worried that exercising joints with OA will cause more joint damage. But regular exercise can actually help reduce some of your symptoms (e.g. pain, stiffness) and improve your joint mobility and strength. It will also move synovial fluid through the joint, providing essential nutrients and removing waste.
Exercises that move your joints through their range of movement will also help maintain joint flexibility; this is often lost due to OA. Strengthening the muscles around your joints is also important. The stronger they are, the more weight they can take. This will help support and protect your joints.
An exercise program that promotes muscle strength, joint flexibility, improved balance and coordination, and general fitness will give you the best results. Start exercising slowly and gradually increase the time and intensity of your exercise sessions over weeks and months. A physiotherapist or exercise physiologist can help you work out an exercise program that’s right for you.
Weight management
Being overweight or obese increases your risk of developing OA and the severity of your condition. The additional weight also increases pressure on your joints, especially your weight-bearing joints (e.g. hips, knees, feet), which is likely to cause further pain and damage.
The amount of overall fat you carry is also significant because fat releases molecules that contribute to low but persistent levels of inflammation across your whole body. This, in turn, increases the level of inflammation in the joints affected by OA.
For these reasons, maintaining a healthy weight is essential if you have OA. Your doctor or dietitian can advise you on safe weight-loss strategies if you need to lose weight.
Weight loss can be a long process for many people. It’s challenging, especially when pain affects your ability to be as active as you’d like. But it’s good to know that any weight loss can reduce your pain and increase your ability to exercise. So making small, achievable changes to your eating and exercise habits can bring big results. It just takes time, commitment, and support.
Medicines
No medicines can affect the underlying disease process of OA, but combined with exercise, weight management, and self-care, medicines may provide temporary pain relief and help you stay active.
The most commonly used medicines for OA are:
- Non-steroidal anti-inflammatory medicines or NSAIDs (e.g. ibuprofen). These medicines are available over-the-counter and with a prescription, depending on their dosage and other ingredients. They come in tablet/capsule form (oral NSAIDs) or as a gel or rub applied directly to the skin (topical). It’s important to note that oral NSAIDs are designed to be taken at low doses for short periods. Always talk with your doctor before starting NSAIDs, as they can have side effects.
- Paracetamol. Research has shown that paracetamol provides only low-level pain relief for osteoarthritis. However, some people report that it helps reduce their pain so they can be more active. For this reason, it’s worth discussing a trial of paracetamol with your GP to see if it‘s appropriate for you.
- Corticosteroid (steroid) injections may be helpful for people who haven’t found relief from other treatments (e.g. exercise, weight loss) or other medicines. Corticosteroid injections into a joint can provide short-term pain relief; however, the number of injections you can have each year is limited due to potential harm.
Note: Opioids are powerful pain-relieving medicines that effectively reduce acute pain (or the pain resulting from an injury or surgery). In the past, they were prescribed to treat pain associated with conditions like osteoarthritis; however, there’s strong evidence that they have little effect on OA pain. Opioids also have many potentially serious side effects. That’s why they’re not recommended in the management of OA. Read the Choosing Wisely Australia resource ‘5 Questions to ask about using opioids for back pain or osteoarthritis’ for more info.
Self-care
There are many other things you can do to reduce the impact of your symptoms, including:
- Learning about your condition. Understanding OA and how it affects you means you can make informed decisions about your healthcare and actively manage it.
- Learning ways to manage your pain. Pain is the most common symptom of osteoarthritis, so it’s crucial to learn to manage it effectively. Read our A-Z guide for managing pain for more information.
- Working closely with your healthcare team. The best way to live well with OA is by working closely with the people in your healthcare team (e.g. GP, physio) and keeping them informed about how you’re doing and alerting them to any changes.
- Protecting your joints. Supports such as walking aids, specialised cooking utensils, ergonomic computer equipment and long-handled shoehorns can reduce joint strain and make life easier. An occupational therapist can advise you on aids, equipment and home modifications. You can also check out our range of aids in our online shop.
- Taping, knee braces and orthotics may be helpful if you have OA in your knees or feet. A physiotherapist or podiatrist can advise you on these.
- Improving sleep quality. Not getting enough quality sleep can worsen your symptoms; however, getting a good night’s sleep when you have osteoarthritis and chronic pain can be challenging. If you’re having problems sleeping, talk with your doctor about ways you can address this.
- Managing stress. Stress can also aggravate your symptoms, so learning to deal with stress is extremely helpful. Things you can do to manage stress include planning your day and setting priorities, using relaxation techniques such as going for a walk, getting a massage or listening to music, and, where possible, avoiding people and situations that cause you stress.
- Eating a healthy, balanced diet. While there’s no specific diet for OA, it’s important to have a healthy, balanced diet to maintain general health and prevent weight gain and other medical problems, such as diabetes and heart disease.
Surgery
In most cases, surgery isn’t required for people with osteoarthritis. However, surgery may be an option if all non-surgical treatment options have been unsuccessful and you’re still experiencing significant pain and loss of function.
The most common surgery for osteoarthritis is a joint replacement. When considering surgery, you should be informed about what it involves, the rehabilitation process, and its potential benefits and risks.
Note: An arthroscopy isn’t recommended to treat knee OA. Evidence shows it’s not effective in improving OA knee pain or function.
Contact our free national Help Line
Call our nurses if you have questions about managing your pain, musculoskeletal condition, treatment options, mental health issues, telehealth, or accessing services. They’re available weekdays between 9am-5pm on 1800 263 265; email (helpline@msk.org.au) or via Messenger.
More to explore
- Osteoarthritis
PainHEALTH - Osteoarthritis
American College of Rheumatology - Osteoarthritis
Arthritis Foundation - Osteoarthritis
healthdirect - Osteoarthritis
Versus Arthritis UK - Patient education: Osteoarthritis symptoms and diagnosis (Beyond the Basics)
UpToDate - Patient education: Osteoarthritis treatment (Beyond the Basics)
UpToDate